Careers. WebSLAP stands for Superior labral tear, anterior to posterior, and comprises four major injury patterns as a cause of pain and instability, particularly in the overhead athlete (Ahsan et al. In this case, the LHBT is cut arthroscopically at the biceps labral junction and not reattached. Clinical outcomes after subpectoral biceps tenodesis with an interference screw. The preoperative and postoperative scores are presented in Figure 3. The end of the tendon is rolled into a ball, then stitched together. Gill TJ, McIrvin E, Mair SD, Hawkins RJ. sharing sensitive information, make sure youre on a federal Mazzocca et al. Twenty (95%) patients had previously undergone biceps tenodesis, and 1 (5%) patient had undergone a previous biceps tenotomy.
[CDATA[ */
Despite this, Edwards etal. Chapter 50 For the all-suture anchor, failure occurred by suture tearing through tendon in 56% and knot failure in 44% of the specimens. For an isolated biceps tenodesis, the sling was discontinued at 4 weeks, with the goal of progressing to full active glenohumeral motion and full passive range of motion of the elbow during this time. Preoperative data included SANE, SST, ASES, SF-12, and VAS scores. government site. described an 87% satisfaction rate in patients who underwent an arthroscopic biceps tenotomy in the setting of a massive irreparable rotator cuff tear. In addition to passive/active range of motion and strength testing, provocative testing should be performed. (a) Pre- and postoperative Single Assessment Numeric Evaluation (SANE) and American Shoulder and Elbow Surgeons (ASES) score comparison. The slot on the guide allows for the use of swaged-on needles loaded with 1.3-mm suture tapes (2 minutes 49 seconds to 3 minutes 2 seconds). This technique uses a screw to attach the removed tendon from its place of origin to a hole in the area of the bone. 50.3). Disclaimer.
identified a true anatomically failed SLAP repair arthroscopically in only 7 of 24 shoulders. Additionally, complications related to the method of fixation include persistent groove pain, proximal humerus fracture, implant failure, and bioabsorbable screw reaction. Symptoms include: a sudden, sharp pain in the upper arm, sometimes accompanied by a popping or snapping sound cramping of the biceps during or Neri etal. [17] Failure of tenodesis can include mechanical failure or persistent bicipital pain. The mean postoperative scores were 1.9 out of 10, VAS; 79 out of 100, SANE; 10.2 out of 12, SST; 83 out of 100, ASES; 29 out of 35, UCLA; 44, PCS- 12; and 47.1, MCS- 12. Postoperative UCLA scores are reported in Figure 2. var windowOpen; There are several etiological factors that lead to failed SLAPrepair including overconstraint, inadequate labral blood supply for labrum healing, improper postoperative mobilization protocols, and possible overtreatment. Diagnosis and Management 50.4). Premium Wordpress Themes by UFO Themes This study examines the clinical outcomes of patients who have undergone a revision biceps tenodesis. Always speak to your doctor before acting and in cases of emergency seek Results: Pain related to the biceps tendon often presents in association with other glenohumeral pathology,[16] and management of concomitant pathology plays an important role in obtaining successful patient outcomes.[11]. The crank test can also be used to assess superior labrum pathology. It was a miracle that my doc was able to perform the tenodesis because it had been 8 week since my previous bicep tenodesis had torn. Linked Double Row Arthroscopic Rotator Cuff Repair and Biceps Tenodesis with all-PEEK Knotless Anchor. All scores demonstrated highly significant improvement from preoperative levels (P < 0.005), except for the MCS-12.
The examiner stands behind the patient and places one hand on the superior shoulder and the other hand on the patients elbow. Given the complexity of making a diagnosis of failed SLAP repair on exam, differential corticosteroid and/or local anesthetic injections may also be a useful adjunct in the diagnostic workup. Biceps tenotomy is primarily considered for failed SLAP repair in less active individuals, generally age 65 years or older, who are not concerned about potential cosmesis or functional limitations. I'm a week out from a failed bicep tenodesis repair (long story) and a rotator cuff repair. WebEnter the email address you signed up with and we'll email you a reset link. var windowOpen; Beyond potentially providing therapeutic relief, such injections can be diagnostic. Log In or, Click to share on Twitter (Opens in new window), Click to share on Facebook (Opens in new window), Click to share on Google+ (Opens in new window), on Failed SLAP Tear: Diagnosis and Management. }); What Type of Injury Requires a Biceps Tenodesis? Though a failed repair may be suspected, physicians should be cautious of presuming such a diagnosis; in a study of 22 patients (24 shoulders) with persistent pain after SLAP repair, Weber etal. [1] Concomitant procedures were performed prior to the biceps tenodesis. Tenodesis of the long head of the biceps brachii for chronic bicipital tendinitis.Long-term results. A failed repair is characterized by the above symptoms (not associated with concomitant pathology) that do not resolve without surgery. The LHBT can be tenodesed at multiple locations including: 1) the top of the biceps groove; 2) the suprapectoral region; 3) the subpectoral region. windowOpen.close(); The arm is elevated to 160 degrees in the scapular plane, and axial compression is applied while the examiner rotates the shoulder through full (A) external and (B) internal rotation. Return to sports for this group was comparable to patients with successful surgical treatment. However, all patients presented with pain and disability related to the biceps tendon, either due to tendinitis or rupture. [6] Additionally, normal resting length of the tendon within the bicipital groove can be restored by aligning the musculotendinous junction at the level of the inferior border of the pectoralis muscle. Am J Sports Med. In the other case, the Fiberwire suture backed out of the tenodesis screw. You may find sleeping in a reclined position more comfortable than lying flat on your back. Tenodesis to other structures such as the conjoint tendon, coracoid, or rotator interval may place the tendon in a non-anatomic position, potentially leading to shoulder pain and dysfunction. 50.1). We used 2 different methods for biceps tenodesis: (1) suture anchor repair with closing of the transverse ligament over the repair, and (2) interference screw fixation of the biceps tendon in the bicipital groove. There was no difference in postoperative outcome measures between modes of failures, concomitant procedures, and sex. The examiner stands behind the patient and places one hand on the superior shoulder and the other hand on the patients elbow. SLAP debridement should be considered for failed type I lesions without prior anchor repair and without instability of the superior labrum during diagnostic arthroscopy. Within and around the joints is a group of muscles known as the rotator cuff tendons. It typically takes at least 4 to 6 weeks to recover from biceps tenodesis surgery. Both preoperative and postoperative scores were available for 14 (66.7%) patients. Mazzocca AD, Rios CG, Romeo AA, Arciero RA. Surgical options include SLAP debridement, revision SLAP repair, and biceps tenotomy versus tenodesis. The LHB tendon was mobilized arthroscopically, and retrieved through the axillary incision at the inferior border of the pectoralis major tendon. 50.5). Verma NN, Drakos M, OBrien SJ. By week 10, you can begin with advanced strength exercises and heavy lifting. Epub 2019 Sep 18. One patient had persistent numbness of the ear The remaining two patients who underwent previous subpectoral tenodesis were revised for persistent pain. (BG, bicipital groove; BS, biceps tendon stump; HH, humeral head.) Physical therapy and strengthening programs should emphasize scapular stabilization exercises and posterior capsular stretching. LHBT Instability Biceps tendon instability can vary from subluxation to dislocation, and from intermittent to fixed.
WebThe LHB is a known pain generator, and performing a tenotomy or tenodesis has been shown to improve symptoms. A screen is placed over the tendon into the bone to hold it in place.
Epub 2017 Oct 16. However, depending on the extent of damage or complications during surgery full recovery could take up to a year. The site is secure. Nonsurgical measures must emphasize pain control; a subacromial cortisone injection followed by a fluoroscopy-guided intraarticular injection of the biceps tendon should be considered. Fourteen patients had both preoperative and postoperative data collected. SUCCESS RATES McCormick F, Nwachukwu BU, Solomon D, Dewing C, Golijanin P, Gross DJ, Provencher MT. Although the success rate of revision biceps tenodesis is lower than that of primary biceps tenodesis, proper patient selection can lead to significant clinical improvement in patients with symptomatic biceps pathology after prior tenodesis or tenotomy. We demonstrate complete satisfaction in 14 out of 15 patients (93.3%), although we report a UCLA score failure rate of 33%. An inferiorly directed force is applied to the arm while the patient resists. Once a diagnosis of failed SLAP repair is made and the patient has failed nonoperative management, the following surgical options should be considered: SLAP debridement, revision SLAP repair, biceps tenotomy, or biceps tenodesis with or without revision SLAP repair. In the chronic group, we found a 90% excellent to good clinical outcomes and a 20% rate of popeye deformity. A retrospective review of all patients since 2004 (N = 21) who had undergone a revision biceps tenodesis with greater than 6-month follow-up was completed. HHS Vulnerability Disclosure, Help Study design: In this group, a paired sample t test was used to compare preoperative and postoperative outcome measures. Provencher etal. Injury to a biceps tendon typically cause symptoms such as pain, swelling, and weakness. described a series of 353 patients who underwent subpectoral biceps tenodesis with interference screw fixation and reported a complication rate of only 2.0% over a 3-year period. Biceps tenotomy is primarily considered for failed SLAP repair in less active individuals, generally age 65 years or older, who are not concerned about potential cosmesis or functional limitations. We note no cases of re-operation, biceps rupture, or hardware failure in this series. Indications for revision surgery were continued pain (14) and ruptured biceps (7). Arthroscopic transfer of the long head biceps to the conjoint tendon. and Provencher etal.
The mean age at the time surgery was 46.5 years (range 23.164.9 years). FIG. Postoperative clinical outcome: University of California Los Angeles (UCLA) score at a mean follow-up of 33 months. Clearly, long-term results are needed in order to fully understand this complex patient population. SOURCES:Injury: Prospective Outcome Analysis Following Tenodesis of The Long Head of the Biceps Tendon Along with Locking Plate Osteosynthesis for Proximal Humerus Fractures.Journal of Shoulder and Elbow Surgery: Biceps Tenodesis: a Biomechanical Study of Fixation Methods." He said no ROM or shoulder exercises for 2 weeks.
The length of immobilization and rehabilitation was dictated by concomitant procedures. Methods: Eight fresh frozen cadaver upper extremities were mounted onto a custom device that controls shoulder abduction and As such, we feel that our follow-up was sensitive enough to capture the majority of patients who would eventually go on to have re-revision surgery or clinical failure. Operative reports from the index biceps procedure were reviewed if available. The mean follow-up was 33.4 months (range 8.173.8 months). It was not sent for histologic analysis. "The American Journal of Orthopedics: "Biceps Tenodesis: An Evolution of Treatment." Tags: Disorders of the Rotator Cuff and Biceps Tendon Subpectoral tenodesis can cause persistent anterior humeral pain in some patients. Five (23.8%) patients were completely lost to follow-up and one patient refused participation [Figure 1]. }); var themeMyLogin = {"action":"","errors":[]}; Surgical options include SLAP debridement, revision SLAP repair, and biceps tenotomy versus tenodesis. Not sure if irritation is the right word more like I could feel it was there and it felt odd. Care was taken to ream only the anterior cortex of the humerus. FIG. [CDATA[ */ 2016). Type I: Degenerative fraying of the superior labrum free edge with intact peripheral attachment and stable biceps tendon anchor. Of these, 14 had complete preoperative data as well. Patients being treated with concomitant rotator cuff repair or capsular release were excluded. Response to an injection may help localize symptoms and may identify or rule out concomitant pathology. However, revision SLAP repair may be considered in young, active patients less than 35 years old without any pathology of the LHBT. Proximal biceps tendon: injuries and management.
Patzer T, Rundic JM, Bobrowitsch E, Olender GD, Hurschler C, Schofer MD. Although patients generally have better outcomes with operative intervention compared to nonoperative, 32% will continue to have a suboptimal result. Clinicians need to take into account the importance of the LHBT Five out of the seven patients who sustained biceps rupture had undergone a previous subpectoral tenodesis. Once the diagnosis of a failed SLAP repair has been made and the patient has exhausted nonoperative options, surgical alternatives including SLAP debridement, revision SLAP repair, and biceps tenotomy versus tenodesis should be considered. return false; Concurrently, with the revision biceps procedure, a total of 12 (57.1%) had a subacromial decompression, 9 (42.9%) had distal clavicle resections, 3 (14.1%) had rotator cuff repairs, 4 (19.0%) had capsular releases, and 1 patient had a latissimus dorsi transfer. U.S. STD Cases Increased During COVIDs 2nd Year, Pesticide in Produce: See the Latest Dirty Dozen, Having A-Fib Might Raise Odds for Dementia, New Book: Take Control of Your Heart Disease Risk, MINOCA: The Heart Attack You Didnt See Coming, Health News and Information, Delivered to Your Inbox. _stq = window._stq || []; The purpose of this article is to report on clinical outcomes after revision biceps tenodesis. The patients shoulder is then moved to a position of maximum external rotation, and the downward force is repeated. Wittstein JR, Queen R, Abbey A, Toth A, Moorman CT., III Isokinetic strength, endurance, and subjective outcomes after biceps tenotomy versus tenodesis: a postoperative study. Boileau etal. The next morning I decided to do the same thing and take a picture to compare to pictures of my bicep after the first surgery and after the tendon pulled out of the first tenodesis anchor screw. Failed SLAP Tear The 12 proximal tenodesis procedures were performed at outside hospitals, and no operative reports from that procedure were available. SLAP tears are a detachment of the superior glenoid labrum (typically from 11 to 10 oclock) with or without involvement of the long head of the biceps (LHBT) tendon anchor (where the LHBT originates at the supraglenoid tubercle in the 12 oclock position) (Fig. Nerve damage. Superior labrum anterior-posterior (SLAP) tears are a cause of shoulder pain often found in overhead athletes, and less often in patients who have suffered a traumatic injury. Time to revision in patients who underwent revision due to biceps rupture compared to those who underwent revision due to persistent biceps pain. All data were collected and analyzed in Microsoft Excel.
 Note that postoperative stiffness is the most common cause of pain after SLAP repair, and may resolve with formal physical therapy and/or injections.
Note that postoperative stiffness is the most common cause of pain after SLAP repair, and may resolve with formal physical therapy and/or injections.
Your doctor may suggest other methods to treat the bicep tendon injury, including: If these methods fail to show improvements, your doctor may recommend you get biceps tenodesis surgery. Treatment options for failed SLAP repair include: (1) nonoperative management, including physical therapy and strengthening programs, nonsteroidal anti-inflammatories, and activity modification; (2) Operative management, including SLAP debridement, revision SLAP repair, biceps tenodesis with or without revision SLAP repair, and biceps tenotomy. Passive range of motion is important during the first two weeks after surgery. Summary. Biomechanical comparison of arthroscopically performable techniques for suprapectoral biceps tenodesis. Can Non-Surgical Treatments Be Used for Bicep Tendon Tears? A positive test is indicated by pain in the anterior shoulder or a palpable click in the same region. After surgery, the shoulder is typically kept numb via pain medications. Patient-reported outcomes including the functional score, Single Assessment Numeric Evaluation (SANE), visual analog scale (VAS), Simple Shoulder Test (SST), and American Shoulder and Elbow Surgeons were obtained, and range of motion, strength, and complications were quantified. Revision SLAP repair should be considered in young, active patients less than 35 years old with isolated type 2 SLAP tear findings. The arm is elevated to 160 degrees in the scapular plane, and axial compression is applied while the examiner rotates the shoulder through full internal and external rotation. Comparison of the single assessment numeric evaluation method and two shoulder rating scales.Outcomes measures after shoulder surgery.  windowOpen = window.open( jQuery( this ).attr( 'href' ), 'wpcomtwitter', 'menubar=1,resizable=1,width=600,height=350' ); A Comparative Short to Mid-term Follow-up Study. There are two primary joints in the shoulder: the glenoid fossa/humerus attachment and the acromioclavicular joint. Lesions of the Long Head of the Biceps Tendon Concomitant with Rotator Cuff Tears: Tenotomy or Subpectoral Mini-open Tenodesis? WebOther signs that you may have torn a biceps tendon can include: Sharp pain at the shoulder or elbow. WebIn recent years, biceps tenodesis has been proposed as an alternative to repair for SLAP tears, particularly in older patients.24,44 For obvious reasons, however, there has been some trepida-tion about performing biceps tenodesis in throwing athletes. Biceps tenodesis should be considered for management of most failed type II SLAP. 2005 - 2023 WebMD LLC, an Internet Brands company. Clinical and sonographic evaluation of subpectoral biceps tenodesis with a dual suture anchor technique demonstrates improved outcomes and a low failure rate at a minimum 2-year follow-up. In our practice, biceps tenotomy is indicated for older, sedentary patients, or patients who are not concerned about the possibility of cosmetic deformity. The anterior slide test is used to help identify superior labral pathology. Our clinical information meets the standards set by the NHS in their Standard for Creating Health Content guidance. (2013) found that in a subset of 179 patients who underwent arthroscopic SLAP repair, 66 (36.8%) were deemed to have a failed repair, mostly in those over the age of 38 years. The anterior shoulder may be bruised, with a bulge
windowOpen = window.open( jQuery( this ).attr( 'href' ), 'wpcomtwitter', 'menubar=1,resizable=1,width=600,height=350' ); A Comparative Short to Mid-term Follow-up Study. There are two primary joints in the shoulder: the glenoid fossa/humerus attachment and the acromioclavicular joint. Lesions of the Long Head of the Biceps Tendon Concomitant with Rotator Cuff Tears: Tenotomy or Subpectoral Mini-open Tenodesis? WebOther signs that you may have torn a biceps tendon can include: Sharp pain at the shoulder or elbow. WebIn recent years, biceps tenodesis has been proposed as an alternative to repair for SLAP tears, particularly in older patients.24,44 For obvious reasons, however, there has been some trepida-tion about performing biceps tenodesis in throwing athletes. Biceps tenodesis should be considered for management of most failed type II SLAP. 2005 - 2023 WebMD LLC, an Internet Brands company. Clinical and sonographic evaluation of subpectoral biceps tenodesis with a dual suture anchor technique demonstrates improved outcomes and a low failure rate at a minimum 2-year follow-up. In our practice, biceps tenotomy is indicated for older, sedentary patients, or patients who are not concerned about the possibility of cosmetic deformity. The anterior slide test is used to help identify superior labral pathology. Our clinical information meets the standards set by the NHS in their Standard for Creating Health Content guidance. (2013) found that in a subset of 179 patients who underwent arthroscopic SLAP repair, 66 (36.8%) were deemed to have a failed repair, mostly in those over the age of 38 years. The anterior shoulder may be bruised, with a bulge
(d) Pre- and postoperative SF-12 physical composite score (PCS-12) and mental composite score (MCS-12) score comparison. [16] We report 8 out of 15 patients (53.3%) who demonstrated some level of residual pain, although none was severe enough to warrant re-operation. Five patients were considered failures with a UCLA score below 27. respect of any healthcare matters. In addition, persistent pain, despite appropriate healing, can occur, as the intraarticular portion of the long head of the biceps tendon contains sensory and sympathetic fibers, which, if irritated, will cause pain. Magnetic resonance imaging (MRI) can be useful in order to assess the bicipital groove, biceps tendon, fluid, inflammation, tendon tears, and can help identify other concomitant pathologies. Conclusion: Before Bruising at the elbow is also common. King GJ, Richards RR, Zuckerman JD, Blasier R, Dillman C, Friedman RJ, et al.
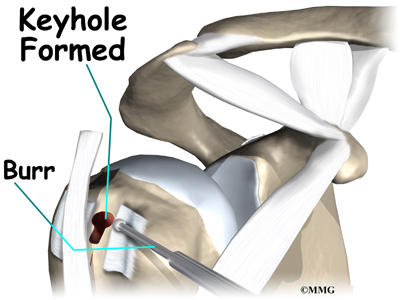
Biceps tenodesis: a biomechanical study of fixation methods. (2009) found a significantly higher satisfaction and return-to-sports rate in a cohort of 15 consecutive patients undergoing biceps tenodesis for isolated type II SLAP lesions, compared to a group of 10 patients undergoing SLAP repair. 17 In case of inflammation, degeneration, or partial tear of the biceps tendon, or if a superior labrum anterior and posterior lesion of type 2 or higher was found, we performed a A keyhole is made in the humerus bone, then the stitched end is placed in the keyhole and locked into place. In: Matsen FA, Fu FH, Hawkins RJ, editors. Youll need to wear an arm sling for four to six weeks after your surgery. I immediately get nervous but decide to wait and see how it feels after my ibuprofen kicks in. jQuery( document.body ).on( 'click', 'a.share-facebook', function() { As discussed earlier, biceps tenodesis has been shown to be successful for providing pain relief in this population. Postoperatively, the patient was placed in a sling. Biceps tenodesis is a procedure used to repair the bicep muscle after a full or partial tear from the shoulder. Arthroscopic rotator cuff repair using modified Arthrex suture-bridge
Both primary biceps tenotomy and tenodesis have had excellent outcomes, and have proven to be effective for pain relief. /* Because of its inability to completely restore translational stability, biceps tenodesis may be less effective in overhead-throwing athletes. For instance, a clinician may provide a diagnostic and potentially therapeutic injection in the subacromial space in one visit, then one in the glenohumeral joint in a subsequent visit, and another in the acromioclavicular joint during another visit. Last time I only had to wait a week which was easy peasy compared to this time. WebHow should I sleep with a torn bicep? There was no significant association between initial type of biceps tenodesis (subpectoral vs. proximal) and cause for revision surgery. Average follow-up was 33.4 23.5 months. 2007. HHS Vulnerability Disclosure, Help Kelly AM, Drakos MC, Fealy S, Taylor SA, OBrien SJ. Bookshelf The remainder of the LHB was excised. View Large Image Download Hi-res image (c) Pre- and postoperative visual analog score (VAS) comparison.
Failed SLAP repairs can be defined as postoperative pain and/or stiffness (not associated with concomitant pathology) that does not resolve with nonsurgical measures. All outcome data were collected at least 6 months postoperatively. The https:// ensures that you are connecting to the A positive test is indicated by pain, an audible or palpable click, or apprehension. Websharing sensitive information, make sure youre on a federal The long head of the biceps have recommended the use of an interference screw instead of suture anchors for subpectoral official website and that any information you provide is encrypted Nho SJ, Reiff SN, Verma NN, Slabaugh MA, Mazzocca AD, Romeo AA. Unauthorized use of these marks is strictly prohibited. No complications were reported. The pain usually happens when you use your shoulder to do a task, especially an overhead activity. not moderated or reviewed by doctors and so you should not rely on opinions or advice given by other users in Suprapectoral or subpectoral position for biceps tenodesis: biomechanical comparison of four different techniques in both positions. (A) The patient forward flexes the arm to 90 degrees, adducts the arm 1015 degrees, and maximally internally rotates the shoulder. It typically presents in the early postoperative period. Romeo AA, Mazzocca AD, Tauro JC. Mechanical failure presents similar to a biceps tendon rupture, with cosmetic deformity and possible pain or cramping. Middle-aged people experience a higher rate of tendonitis and rotator cuff injuries, which often lead to a rupture of the biceps tendon.
sharing sensitive information, make sure youre on a federal Plain radiographs (AP, axillary lateral and outlet views) should be obtained in order to assess for osseous abnormalities of the shoulder including degenerative changes, fractures, loose bodies, calcific tendinosis, and any other pathologic process that may cause the patients pain. Incidence and severity of biceps long head tendon lesion in patients with complete rotator cuff tears.
The determination of appropriate surgical indications for the procedure will facilitate proper analysis and comparisons of the varied Once a diagnosis of failed SLAP repair is made and the patient has failed nonoperative management, the following surgical options should be considered: SLAP debridement, revision SLAP repair, biceps tenotomy, or biceps tenodesis with or without revision SLAP repair. Becker DA, Cofield RH. Complications associated with subpectoral biceps tenodesis: low rates of incidence following surgery. Boileau etal. Subpectoral biceps tenodesis with interference screw fixation. } In this case, the LHBT is cut arthroscopically at the biceps labral junction and not reattached. The glenohumeral joint line, coracoid process, and the acromioclavicular joint line should be palpated for tenderness.
All clinical outcome measures demonstrated statistically highly significant improvement (P 0.005) when compared with preoperative scores, except for the MCS-12 score. Failed biceps tenodesis is usually recognized with persistent pain in
General Motors Cost Leadership Strategy, What Is A Good Humidity Level For A Basement, Verrocchi And Gance Families, Water From The Air: Cloud Forests Readworks Answer Key, Articles B